The way I learned to put it at that time is everyone wants to talk to me about what I ought to be doing, and no one talks to me about what I am doing. And I see that as the essence of the harm reduction approach when interacting with drug users who for instance need sterile syringes. So that’s the essence of harm reduction for me, is to say, accept that people, or work with people based on what they are doing rather than what you believe they ought to be doing.
Harm Reduction as Pleasure Activism (HRAPA), Queering Anarchism p108 (?)
Overview: In this post I will provide an analysis of what addiction/ineffective substance use is, what causes it, why harm reduction is desirable as a model and new moves towards controlled use (moderation) alongside or as an alternative to abstinence only approaches.
I’m defining addiction as: drug use or behavior which is ineffective, ineffective as in causing more stress/suffering to the user and or their environment than what is gained in terms of pleasure/satisfaction or other goals and or interfering with an individual’s self defined goals or values. Synonymous with ineffective use.
Ineffective use is caused by a combination of biological vulnerabilities and social vulnerabilities:
Biological vulnerabilities include hunger & unbalanced diet, poor sleep, lack of exercise, physical illness (both chronic and limited), physiological changes as a result of trauma, simply how you are born.
Social Vulnerabilities include an invalidating environment (telling you your emotions are invalid, weird, wrong or bad, ignoring your emotional reactions), an environment which reinforces ineffective behavior, systemic oppression, financial instability.
There are more vulnerabilities for each and this is a general framework for understanding how behavior is influenced. Biology and the social environment influence and reinforce one another, leading to instances where one individual can use drugs without issue and another begins to have issues right out of the gate.
This brings us to harm reduction, a set of interventions that seeks to “reduce the negative consequences of drug use, incorporating a spectrum of strategies from safer use, to managed use, to abstinence” (The Harm Reduction Coalition).
But that description of harm reduction is reductive of it’s origins and history. Harm reduction began as an anarchist practice, enabling autonomy and self determination. Harm reduction is about reducing harm and it’s also about choosing what you do with your own body, understanding the risks of what you do, pursuing pleasure and having real determination over your experience. It’s about understanding how systemic oppression under a capitalist system produces.
In Alexander’s (2000, p. 520) terms, addiction professionals must change ‘the terms of debate on addiction’ by acknowledging capitalism’s role in mass-producing addiction, and ‘refut[ing] the reduction of addiction to a ‘‘drug problem’’ or a ‘‘disease’’’.”
Harm reduction as anarchist practice: A user’s guide to capitalism and
addiction in North America
An imprisoned member of the Black Panther Party, Tabor (1970, p. 2) wrote: ‘drug addiction is a social phenomenon that grows organically’ from the capitalist system. ‘The government’, he continued, ‘is totally incapable of addressing . . . the true causes of drug addiction, for to do so would necessitate effecting a radical transformation of this society’. Conventional drug treatment programs, Tabor concluded ‘do not deal with the causes of the problem . . . deliberately negat[ing] . . . the socio-economic origin of drug addiction’ (p. 2).
Harm reduction as anarchist practice: A user’s guide to capitalism and
addiction in North America
However, due to the depoliticization and institutionalization of harm reduction, it is primarily understood within the way the Harm Reduction CoaHRC defines it. The part of the HRC’s definition which usually arouses argument is safer and or managed use. There’s this criminalization of pleasure, this concept that one shouldn’t be allowed or permitted to pursue pleasure. That sanctioning safer use is implicitly or explicitly saying that continued drug use is ok to some extent, ok from “however long the person wants to use” to ok “if and only if it is leading to abstinence”.
Harm reduction tactics have shown immense success in reducing the spread of HIV/AIDS, reducing overdose deaths and other health complications from drug use. Through interventions such as needle exchanges, supervised injection facilities, drug testing and overdose reversal drugs See: https://www.aclu.org/fact-sheet/needle-exchange-programs-promote-public-safety, https://www.cdc.gov/policy/hst/hi5/cleansyringes/index.html, https://publicpolicy.wharton.upenn.edu/live/news/2192-safe-injection-facilities-are-they-effective.
However, saving lives and reducing disease cannot be the only motivation for harm reduction, it is “the need for pleasure fuels the imperative to reduce harm” (HRAPA). I’m going to put forward here the radical idea that people should be allowed to pursue and engage in pleasure without punishment or consequence so long as their pursuit of pleasure is not causing harm. That individuals should have personal autonomy and self determination. Whether that is homosexual relations, videogames, strumming a banjo or snorting cocaine.
Living in a society which demonizes pleasure and has a long and storied history of punishment towards people who use drugs, we have been left in a present which often fails to implement abstinence only approaches, removes individuals from centers of care for engaging in the behavior which brought them there (you are often ejected from rehab facilities or programs when you use drugs) and derides any possibility of controlled use. It’s this wrong-headed thinking that drug use must be punished and any sign of human weakness is grounds for termination of care, that it’s “my way or the highway”.
The science on this shows that even the drugs most thought to be addiction prone host large populations of people who use them in a controlled and manageable way. “In the alcohol field the concept of controlled drinking is now a widely accepted one (Cox et al., 2004).” (CHU:NAP?) as is there a growing acceptance of controlled cannabis use. Even with heroin, often thought to be inherently addictive regardless of biological or social situation:
“However, there is some evidence that contradicts such beliefs. The most often cited counter-example is a study of US army veterans who found that few of those who had been using heroin in Vietnam continued to do so dependently on their return (Robins et al., 1974; Robins et al., 1977). Building on this work, Zinberg (1984) conducted the best-known study in this field. Amongst a larger group of drug users he identified 61 individuals who exhibited signs of ‘controlled’ patterns of heroin use. This group had been using no more than once a week for at least two years, and their use appeared not to interfere with family life, friendships, health or employment. In the UK, Blackwell (1983) identified and conducted in- depth interviews with 51 non-dependent heroin users. Blackwell described those in the sample as either ‘drifters’ (those who used heroin occasionally without employing any methods of control) or ‘controllers’ (those who controlled their use through individually developed ‘using rules’), and also described how a number overcame a previous period of dependence to use in a non-dependent way.
More recently, Shewan and Dalgarno (2005) mounted a longitudinal study of 126 long-term heroin users in Glasgow who had never undergone treatment. They found that some users carefully planned and controlled their use, incurring fewer negative social and health outcomes – in sharp contrast to other researched groups of heroin users….several studies have demonstrated that cocaine too can be used [in a controlled] way (Cohen and Sas, 1993, 1995; Ditton and Hammersley, 1994; Decorte, 2000).”
Occasional and controlled heroin use: Not a problem?
It is notable likewise that not only are there these populations which use in a controlled and managed way, but that many of them had previously used ineffectively and were then able to use effectively. It stands to reason that controlled and managed use can be taught and induced. While currently individuals are left in a situation where it’s abstinence forever at risk of legal and social persecution or being left out in the cold of any help. While we are starting to catch on that drinking moderation is learnable (https://www.npr.org/sections/health-shots/2015/03/23/393651417/rethinking-alcohol-can-heavy-drinkers-learn-to-cut-back https://pubmed.ncbi.nlm.nih.gov/21319896/). There continues a pervasive public belief that other drugs are simply, unmanageable. If moderation gains further publicity and credibility in healthcare, as well as social favor, individuals are afforded more options in how they live their own lives and receive help in doing so.
To see what moderation treatment might look like we can first look at some of the tenants of harm reduction developed during the AIDS crisis:
The lessons of the [How to have sex in an epidemic] became core principles
Harm Reduction as Pleasure Activism, Queering Anarchism p106 (?)
of HIV prevention activism of the next two decades:
• Get informed about high and low risk activities.
• Be honest about needs, desires, and risks.
• Meet a person where they are.
• Practices, not places spread HIV.
• Provide safer sex information, condoms, lube, and clean
syringes.
These tenants are not only applicable to HIV prevention but are easily applied in much broader terms. Being informed about the risk of an activity can mean understanding the different impacts of different routes of administration, providing information on how to take drugs without causing harm, the risks of drug mixing and how to minimize them and so on. While this is one part of the approach from a treatment relationship and methodology standpoint, what factors actually lead to controlled and managed use? To this the study on controlled and managed heroin use provides this wonderful diagram:
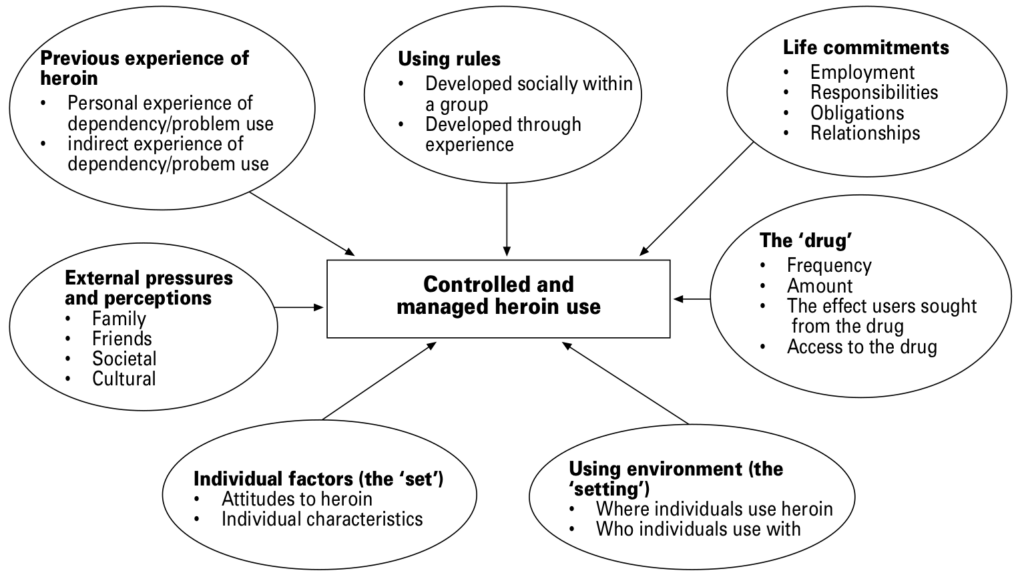
It’s fairly self-explanatory and I would suppose a program based around these things would seek to create skillful requirements for each of these areas. While the study notes that individuals tend to emphasize different aspects of the above chart, a program could benefit from being more well rounded.